Introduction: New Pressures on Long-Term Care
Though the COVID-19 outbreak has drawn attention to (and amplified) the pressures facing Ontario’s long-term care (LTC) workers, the province’s LTC staffing crisis—and the structural problems contributing to it—existed long before the novel coronavirus emerged.1 Workers and employers across the province warned of widespread staffing shortages, low attraction and retention of quality workers, declining wages, worker dissatisfaction, and burnout. The shortage of personal support workers (PSWs), the most numerous group of frontline workers in LTC homes and the group responsible for the majority of hands-on care, is particularly acute.
But why is this happening? What are the long-term structural causes that contributed to the massive challenges facing the system today? In this paper, we provide an overview of the structural challenges to PSW funding that have contributed to the current staffing crisis in Ontario’s LTC homes.
Labour Market Challenges
Demand for PSWs in the LTC sector is extremely high: in a survey by the Ontario Long-Term Care Association, nine in ten homes reported challenges recruiting staff—and PSW positions were the hardest ones to fill.2 This demand will only increase as the 15,000 new LTC beds promised by the Ontario government begin operation.3 And the COVID-19 crisis has led not just to shortages but to a genuine crisis for PSWs, a crisis so acute that the government has created a staffing strategy to address it. The expected response of a labour market, however, where labour shortages in a competitive environment result in higher wages, is prevented by a combination of the government’s failure to properly account for increased resident acuity in LTC funding, a broken arbitration system, a centralized bargaining pattern, and concentrated market actors.
Resident Acuity in LTC has Skyrocketed
In 2010, Ontario expanded its Aging at Home Strategy, designed to keep seniors in their homes or communities longer and to lessen the burden on hospitals of patients needing extended care.4 Since then, stricter admission requirements for entry into LTC homes have been in effect. While LTC facilities have always provided care for residents who needed more support than they could receive at home, now only those with high and very high needs are eligible for admission into LTC. In addition, downloading of responsibilities from hospitals to LTC has meant that high-acuity patients who formerly would have received care in hospitals now receive care in LTC facilities.5 As a result of these transformations in seniors’ care, more residents have been entering LTC at a later stage of their physical and cognitive decline. While there may be sound public-policy reasons for this shift, the requisite changes to staffing that are required to properly handle this increased acuity have not been made.
Envelope Structure of Government Funding Fails to Meet Rising Care Needs with More Staff
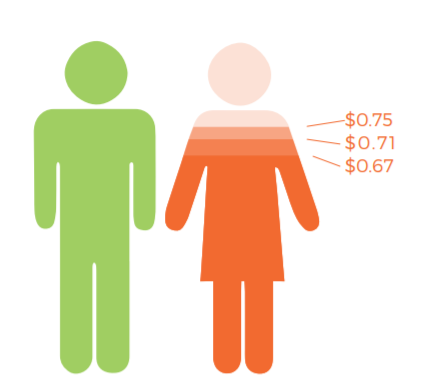
While LTC residents are responsible for some of their room-and-board costs, LTC homes get most of their funding from the government. This funding is administered through four envelopes: nursing and personal care (which includes funding for PSW wages), program and support services, raw food (ingredients for resident meals), and other accommodation. For-profit homes are only allowed to keep—that is, earn a profit from—any surplus funds from the other accommodation envelope. Not-for-profit and municipal homes, meanwhile, keep nothing and have an incentive to reinvest every extra dollar into improving operations and staffing. Given that for-profit homes have an incentive to put surplus funds toward shareholder dividends rather than resident care—and that “one of the principal mechanisms for generating profit is reducing staffing levels, which results in inferior quality of care”6 —it is unsurprising that research has linked for-profit ownership to poorer outcomes for residents in LTC.7 Yet the issues we outline in this paper are not unique to for-profit homes. While there are those who are calling for a removal of for-profit homes from Ontario, this will do little to solve the underlying, structural issues with LTC and its labour-market challenges.
The amount of funding each LTC home receives in its nursing and personal care envelope is calculated accorded to the home’s level of acuity, known as its Case Mix Index (CMI).8 In theory, this system directs funds where they are most needed, by providing more funding to homes whose residents have more complex health problems and thus higher care needs. In practice, however, total provincial funding for the nursing and personal care envelope has not kept pace with the increased staffing demands created by rising acuity in all Ontario LTC homes. A home’s CMI compares the acuity of its residents only to that of other homes in the province each year. It was originally designed to account for increased acuity over time in the system as a whole, but is re-indexed every year to prevent LTC funding from going over budget. Having the same CMI over time results in receiving inflation-adjusted decreases in many of the funding years since 2004. When coupled with the skyrocketing acuity of LTC residents, insufficient funding increases mean that homes are forced to provide more care with less money every year.
The CMI-adjusted funding system also creates a moral dilemma for PSWs and other care staff: if they do not prioritize paperwork over patient care—even if information on some forms was already entered by other staff—the documented acuity of their facility could decrease and cause their home to lose funding in the care envelope, making it even harder to meet patients’ care needs in the future.9 Partial and inconsistent access to technology is a common cause of documentation redundancy: if there aren’t enough tablets to go around, some PSWs have to do mandatory charting using paper at the bedside, leaving the information to be re-entered into the digital system later. Documentation is an important part of care, but every minute that a PSW is forced to spend on redundant or unnecessary paperwork takes away from direct, hands-on resident care. One way to address this in the short term and introduce greater accountability on expanding resident needs would be to pay for charting/documentation costs out of the housing envelope rather than the care envelope. When residents receive less hands-on care, their health and quality of life suffers—a deeply distressing cycle for the many workers who entered LTC to help residents.10
Broken Arbitration System Prevents Unions from Securing Fair Wages
The legal framework for collective bargaining in the LTC sector limits the tools for unions and employers to respond to labour-market pressures. Like hospitals, police forces, and other essential services, LTC homes are not allowed to use strikes and lockouts, meaning that the only option for settling labour disputes is binding arbitration: the opposing parties hire an arbitrator to review their case and agree to accept the arbitrator’s decision for their collective agreement.11 Unlike police forces, however, LTC homes have middle men—facility owners in the role of employers—who act as the actual bargaining partners in labour negotiations, while the payer—the government, which controls funding—is in the background. In other disputes involving essential workers (police officers, firefighters, hospital employees), it is the payer who sits across the table from worker representatives. But in LTC, the employers are simply the administrators of funds, with no direct levers to increase funding. This middle-man system makes it difficult to hold either the payer or the employer accountable for results: employers can (rightly) insist that they don’t control funding, while government is hidden from view throughout the process.